Two Breakthroughs in Pancreatic Cancer: The Toripalimab-AG and PAAG Regimens — Chinese Innovation in Immunotherapy Combinations
Pancreatic ductal adenocarcinoma (PDAC) has long been known as the “king of cancers” — a disease that resists treatment, evades the immune system, and claims lives with a five-year survival rate below 13%. For years, systemic therapy for advanced pancreatic cancer was limited to gemcitabine-based or FOLFIRINOX chemotherapy regimens, with survival gains measured in weeks.
Over the past five years, two pioneering Chinese research teams have independently demonstrated that rationally combining immunotherapy with chemotherapy can meaningfully improve outcomes for this devastating disease. Their work traces an elegant evolutionary arc: from a three-drug combination that first proved the concept, to a four-drug regimen that builds on the initial insight by adding antiangiogenic therapy.
This article reviews both breakthroughs in detail — the toripalimab-AG regimen (2021 ASCO, Prof. Cao Dan’s team) and the PAAG regimen (2026 ASCO, Prof. Du Juan’s team) — and examines how their combined contributions are reshaping the first-line treatment landscape for metastatic pancreatic cancer.
A Visual Overview
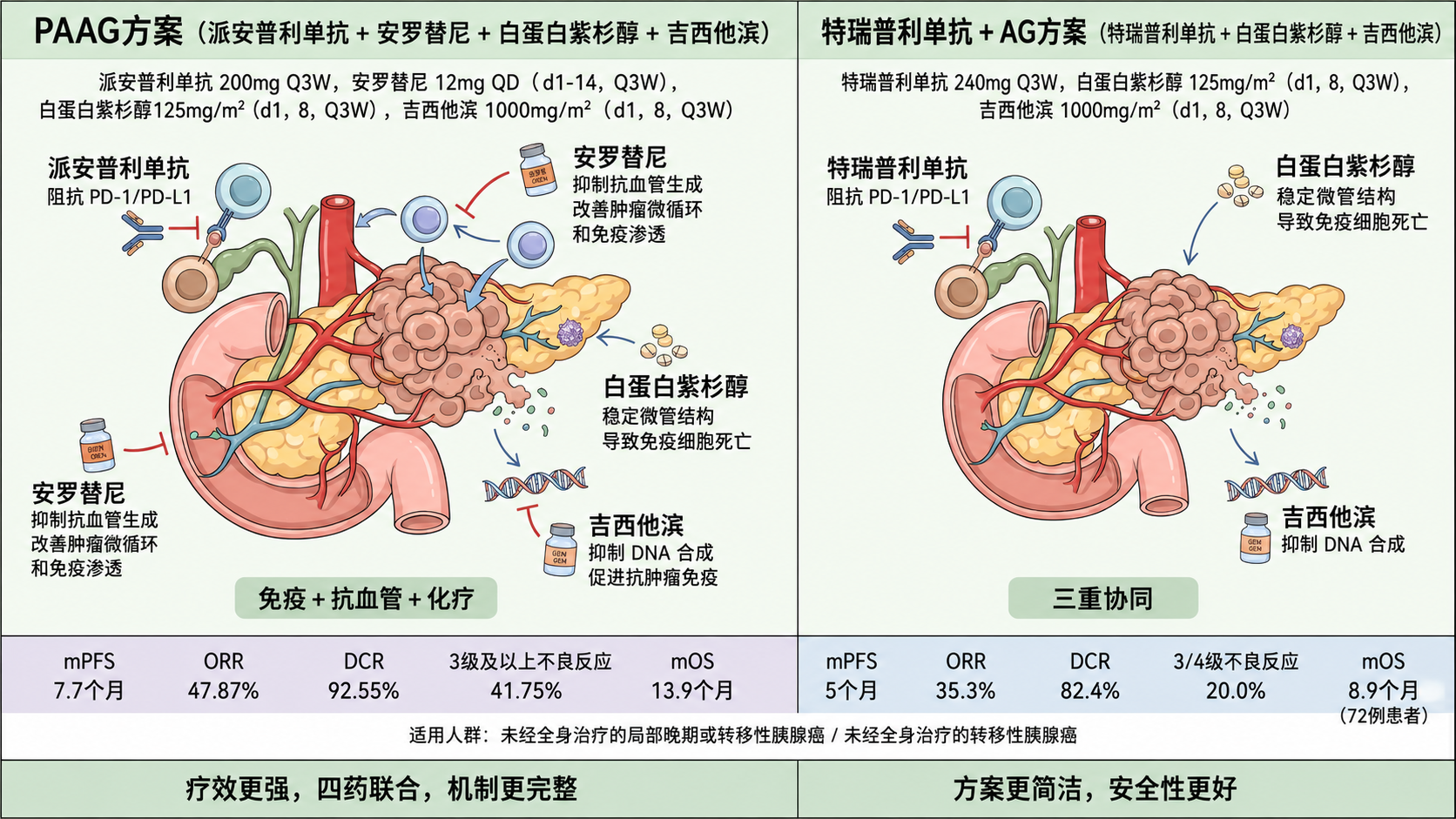
The PAAG quadruplet regimen compared to the toripalimab-AG triplet approach:

Chinese-language comparison chart:
Background: Why Pancreatic Cancer Is a “Cold Tumor”
Pancreatic cancer presents unique challenges for immunotherapy:
- Dense desmoplastic stroma: A thick fibrous barrier that prevents immune cells from reaching cancer cells.
- Immunosuppressive microenvironment: Rich in regulatory T cells (Tregs), myeloid-derived suppressor cells (MDSCs), and M2 macrophages that actively suppress antitumor immunity.
- Aberrant tumor vasculature: Chaotic blood vessels create hypoxic conditions that further suppress T-cell function.
- Low tumor mutational burden (TMB): Few neoantigens mean fewer targets for the immune system to recognize.
These characteristics make pancreatic cancer one of the most immunologically “cold” solid tumors — and the reason why PD-1 inhibitors alone have shown minimal benefit in unselected pancreatic cancer patients.
Both Chinese regimens address these challenges through rational drug combinations rather than single-agent immunotherapy.
Regimen One: Toripalimab + AG (The “Triplet” Approach)
Study Overview
| Field | Details |
|---|---|
| Lead Investigator | Prof. Cao Dan (曹丹), West China Hospital, Sichuan University |
| Published at | ASCO 2021 (preliminary data); Signal Transduction and Targeted Therapy 2024 (final results) |
| Design | Open-label, single-center, single-arm Phase Ib/II trial |
| Enrollment | 20 patients (2021 ASCO preliminary report); 72 patients (final publication) |
| Population | Untreated unresectable locally advanced or metastatic pancreatic ductal adenocarcinoma, ECOG PS ≤ 2 |
Composition: Three Mechanisms in One Regimen
| Component | Dose | Mechanism |
|---|---|---|
| Toripalimab (特瑞普利单抗) | 240 mg IV on Day 1 | Anti-PD-1 immune checkpoint inhibitor — releases the T-cell immune brake |
| Nab-paclitaxel (白蛋白紫杉醇) | 125 mg/m² IV on Days 1, 8 | Disrupts tumor stroma, induces immunogenic cell death |
| Gemcitabine (吉西他滨) | 1000 mg/m² IV on Days 1, 8 | Inhibits DNA synthesis, depletes regulatory T cells |
Cycle: Every 3 weeks.
Key Results
Preliminary Data (2021 ASCO, 20 Patients)
| Endpoint | Result |
|---|---|
| ORR (Objective Response Rate) | 35.3% (6/17 evaluable; 1 CR, 5 PR) |
| DCR (Disease Control Rate) | 82.4% (14/17) |
| Median PFS | 5.0 months (95% CI: 4.216–5.784) |
| 6-month PFS Rate | 60% |
| Median OS | 14.0 months (95% CI: 9.445–18.555) |
| 1-year Survival Rate | 80% |
| Grade 3-4 Adverse Events | 20.0% (4/20) |
Final Published Results (72 Patients, 2024)
| Endpoint | Result |
|---|---|
| ORR | 33.3% (24/72) |
| DCR | 90.3% (65/72) |
| Median PFS | 5.6 months |
| Median OS | 8.9 months |
| 1-year Survival Rate | 31.9% |
| Most Common Toxicities | ALT elevation (35%), leukopenia (30%), metabolic disorders (25%), hypothyroidism (25%) |
Biomarker Findings
The toripalimab-AG study identified several important insights:
- PD-L1 expression and TMB: Efficacy was independent of PD-L1 levels and tumor mutational burden — confirming that traditional immunotherapy biomarkers have limited predictive value in pancreatic cancer.
- Genetic landscape: All patients had mismatch repair proficiency (pMMR); KRAS mutations were present in 90%, TP53 mutations in 90%, and ARID1A mutations in 20%.
- Spatial immune interactions: The interaction pattern between dendritic cells (DC), T helper cells (Th), and cytotoxic T lymphocytes (CTL) in the tumor microenvironment emerged as a strong predictor of response (AUC = 0.8).
Clinical Significance
The toripalimab-AG regimen was the first to demonstrate that adding a PD-1 inhibitor to standard AG chemotherapy could achieve meaningful tumor shrinkage in pancreatic cancer — with an ORR of ~35% that exceeded the historical AG chemotherapy benchmark (~25-28%). More importantly, the preliminary median OS of 14 months exceeded the historical AG chemotherapy median OS of approximately 8.5 months, suggesting that immunotherapy combination could extend survival beyond what chemotherapy alone achieves.
The relatively low rate of grade 3-4 adverse events (20% in the preliminary cohort) indicated that the triplet combination was well-tolerated, laying the foundation for exploring even more ambitious four-drug regimens.
Regimen Two: PAAG (The “Quadruplet” Approach)
Study Overview
| Field | Details |
|---|---|
| Lead Investigator | Prof. Du Juan (杜娟), Nanjing Drum Tower Hospital, Nanjing University Medical School |
| Published at | 2026 ASCO Gastrointestinal Cancers Symposium |
| Clinical Trial ID | NCT06051851 |
| Design | Randomized controlled trial (PAAG vs. standard AG) |
| Enrollment | 155 patients in ITT population (PAAG: 103, AG: 52) |
| Population | Untreated metastatic pancreatic ductal adenocarcinoma, ECOG PS ≤ 2 |
| Data Cutoff | October 31, 2025 |
Composition: Adding Antiangiogenic Therapy to the Mix
| Component | Dose | Mechanism |
|---|---|---|
| Penpulimab (派安普利单抗) | 200 mg IV on Day 1 | Anti-PD-1 immune checkpoint inhibitor — distinct from toripalimab in molecular structure |
| Anlotinib (安罗替尼) | 12 mg orally daily, Days 1-14 | Multi-target antiangiogenic TKI (VEGFR, PDGFR, FGFR, c-Kit) — normalizes tumor vasculature, “starves” the tumor |
| Nab-paclitaxel (白蛋白紫杉醇) | 125 mg/m² IV on Days 1, 8 | Disrupts tumor stroma, induces immunogenic cell death |
| Gemcitabine (吉西他滨) | 1000 mg/m² IV on Days 1, 8 | Inhibits DNA synthesis, promotes antigen presentation |
Cycle: Every 3 weeks. Note that anlotinib is administered Days 1-14 with a 7-day rest period.
Key Results (PAAG vs. Standard AG)
| Endpoint | PAAG Regimen | Standard AG | Improvement | P-value |
|---|---|---|---|---|
| Median PFS | 7.7 months (95% CI: 6.7–8.7) | 4.5 months (95% CI: 3.3–5.8) | +71% | P < 0.001 |
| Median OS | Not reached | Not reached | Data maturing | — |
| ORR (evaluable) | 47.87% (94 evaluable) | 28.57% (49 evaluable) | +68% | P = 0.026 |
| DCR (evaluable) | 92.55% | 67.35% | +37% | P < 0.001 |
| Grade ≥3 AEs | 41.75% | 38.46% | Comparable | P = 0.694 |
| Any-grade AEs | 93.20% | 94.23% | Comparable | P = 1.000 |
Notable: Zero treatment-related deaths in either arm.
The Rationale for Adding Anlotinib
The PAAG regimen adds anlotinib — a domestically developed multi-target tyrosine kinase inhibitor — to the immunotherapy-chemotherapy backbone. This is not a simple addition; it addresses a specific bottleneck in pancreatic cancer immunotherapy:
-
Vascular normalization: Anlotinib inhibits VEGFR, PDGFR, and FGFR, reducing the chaotic tumor vasculature that creates hypoxic, immunosuppressive conditions. Normalized vessels allow immune cells to better infiltrate the tumor.
-
Tumor microenvironment remodeling: Antiangiogenic therapy reduces MDSCs and M2 macrophages while promoting T-cell infiltration — effectively converting a “cold” tumor toward a “hot” one.
-
Direct anti-tumor effects: Beyond its immunomodulatory role, anlotinib disrupts tumor blood supply, contributing to disease control through complementary mechanisms.
Clinical Significance
The PAAG regimen achieves a median PFS of 7.7 months — a 71% improvement over standard AG chemotherapy — with an ORR approaching 48%. The disease control rate of 92.55% means that nearly all evaluable patients experienced either tumor shrinkage or disease stabilization.
Critically, these efficacy gains were achieved without a statistically significant increase in severe adverse events (41.75% vs. 38.46%, P = 0.694), suggesting that adding penpulimab and anlotinib to standard chemotherapy is a tolerable strategy. The most common grade 3 toxicity was leukopenia, consistent with the chemotherapy backbone.
Side-by-Side Comparison
| Feature | Toripalimab-AG (Cao Dan) | PAAG (Du Juan) |
|---|---|---|
| Year | 2021 ASCO (preliminary); 2024 final publication | 2026 ASCO GI |
| Team | West China Hospital, Sichuan University | Nanjing Drum Tower Hospital, Nanjing University |
| Drugs | 3 (toripalimab + AG) | 4 (penpulimab + anlotinib + AG) |
| PD-1 Inhibitor | Toripalimab 240mg D1 | Penpulimab 200mg D1 |
| Anti-angiogenic | None | Anlotinib 12mg D1-14 |
| Design | Single-arm Phase Ib/II | Randomized controlled trial |
| Sample Size | 72 patients (final) | 155 patients (ITT) |
| ORR | 33.3% (24/72) | 47.87% (94 evaluable) |
| DCR | 90.3% (65/72) | 92.55% |
| Median PFS | 5.6 months | 7.7 months |
| Median OS | 8.9 months | Not reached |
| Grade 3-4 AEs | 20.0% (preliminary cohort) | 41.75% |
| Key Insight | First proof that PD-1 + AG works in PDAC; DC-Th-CTL spatial interaction predicts response | Adding antiangiogenic therapy further improves PFS and ORR without proportional toxicity increase |
Critical Distinctions
Different PD-1 inhibitors: The two regimens use different domestic PD-1 inhibitors — toripalimab (toripalimab-AG) and penpulimab (PAAG). These are distinct molecules with different molecular structures and pharmacokinetic profiles, both developed by Chinese pharmaceutical companies.
The anlotinib difference: The presence or absence of anlotinib is the defining structural difference between the two approaches. PAAG explicitly targets the tumor vasculature as a third therapeutic axis, creating a more complex but potentially more effective combination.
Study design: The toripalimab-AG study was a single-arm trial, while the PAAG study used a randomized controlled design — providing a higher level of evidence for the PAAG regimen’s efficacy claims.
The Evolutionary Arc: From Proof of Concept to Optimization
These two studies are best understood not as competing approaches but as sequential milestones in the evolution of pancreatic cancer immunotherapy:
Step 1 — Cao Dan’s triplet (2021): First demonstrated that adding a PD-1 inhibitor to AG chemotherapy could produce meaningful tumor shrinkage in pancreatic cancer. The ~35% ORR and ~5-month PFS exceeded chemotherapy benchmarks, proving the concept that immunotherapy combinations are viable in this “cold” tumor.
Step 2 — Du Juan’s quadruplet (2026): Built on this foundation by asking the critical follow-up question: “What if we normalize the tumor vasculature to help immune cells reach the tumor?” The addition of anlotinib pushed PFS to 7.7 months and ORR to 47.87%, validating the hypothesis that antiangiogenic therapy enhances immunotherapy efficacy in pancreatic cancer.
This progression mirrors a broader trend in oncology: the most effective combinations are not created by random drug stacking but by addressing sequential biological barriers — first overcoming immune suppression (PD-1 blockade), then improving immune cell access (antiangiogenic therapy).
Clinical Implications for Patients
What This Means in Practice
For patients with newly diagnosed metastatic pancreatic cancer, these two Chinese regimens offer:
-
A meaningful PFS advantage: Both regimens extend progression-free survival beyond standard AG chemotherapy (5.6 months and 7.7 months vs. 4.5 months for AG alone).
-
High disease control rates: DCR of ~90-93% means the vast majority of patients experience tumor stabilization or shrinkage, preserving quality of life and creating windows for subsequent therapies.
-
Biomarker-independent access: Unlike KRAS inhibitors or PARP inhibitors that require specific genetic mutations, both regimens are applicable to all comers — making them accessible without the need for molecular profiling delays.
-
Manageable safety profiles: Neither regimen shows a dramatic increase in severe toxicity compared to standard chemotherapy, which is critical for maintaining treatment adherence and quality of life in patients who are often physically frail.
Remaining Questions
- Mature OS data: The PAAG study’s median OS has not yet been reached, and the toripalimab-AG final OS (8.9 months) was lower than the preliminary report (14.0 months). Continued follow-up is essential.
- Head-to-head comparison: No trial has directly compared the triplet and quadruplet approaches.
- Phase III validation: Large-scale confirmatory trials are needed to establish either regimen as a definitive standard of care.
- Global applicability: Both studies enrolled predominantly Chinese populations. Validation in diverse patient groups will be important for international adoption.
Broader Context: NCCN Guidelines and Global Landscape
As of the 2026 NCCN Guidelines for Pancreatic Adenocarcinoma (v2.2026), the first-line systemic therapy options for metastatic disease remain:
- NALIRIFOX (based on NAPOLI-3 Phase III, median OS 11.1 months)
- Nab-paclitaxel/gemcitabine (AG)
- FOLFIRINOX (for patients with good performance status)
- Gemcitabine alone or 5-FU-based regimens (for patients with intermediate performance status)
The PAAG and toripalimab-AG regimens represent emerging evidence that immunotherapy-based combinations are beginning to challenge the traditional chemotherapy-only paradigm. While these regimens have not yet been incorporated into NCCN guidelines, the data presented at ASCO 2026 have generated significant interest in the international community.
Notably, the PAAG regimen’s randomized design places it on a trajectory to potentially influence future guideline updates, particularly if mature OS data confirms the PFS benefit translates into overall survival gains.
Conclusion: A New Era of Rational Combination Therapy
The toripalimab-AG and PAAG regimens represent two chapters in a rapidly evolving story:
-
Toripalimab-AG (Prof. Cao Dan) provided the proof that PD-1 blockade + chemotherapy can work in pancreatic cancer, achieving an ORR of ~35% and establishing that the immunological “coldness” of pancreatic cancer is not an insurmountable barrier.
-
PAAG (Prof. Du Juan) built on this foundation by adding antiangiogenic therapy to further remodel the tumor microenvironment, pushing PFS to 7.7 months and ORR to 47.87% in a randomized controlled design.
Together, these studies demonstrate that Chinese clinical oncology teams are not merely participating in global cancer research — they are leading it, generating original hypotheses, developing domestically produced therapeutics, and producing practice-changing evidence that is reshaping how the world thinks about treating one of medicine’s most intractable diseases.
As the pancreatic cancer field enters an era of unprecedented therapeutic diversity — with KRAS inhibitors, cancer vaccines, CAR-T cells, and novel immunotherapy combinations all advancing simultaneously — the legacy of these two Chinese regimens will be their demonstration that intelligent, biology-driven drug combination is the path forward for diseases that have long defied single-agent therapy.
References
-
Cheng K, Li X, Lv W, et al. Spatial Interactions of Immune Cells as Potential Predictors to Efficacy of Toripalimab Plus Chemotherapy in Locally Advanced or Metastatic Pancreatic Ductal Adenocarcinoma: A Phase Ib/Ii Trial. Signal Transduction and Targeted Therapy. 2024;9(1):321. doi:10.1038/s41392-024-02031-8.
-
Du J, Tong F, Sha H, et al. First-Line Penpulimab and Anlotinib with Nab-Paclitaxel/Gemcitabine (PAAG) in Metastatic Pancreatic Cancer: A Prospective, Multicentre, Biomolecular Exploratory, Phase II Trial. Signal Transduction and Targeted Therapy. 2024;9(1):143. doi:10.1038/s41392-024-01857-6.
-
Du J, Tong F, Sha H, et al. Penpulimab combined with anlotinib and nab-paclitaxel plus gemcitabine (PAAG) as first-line treatment for metastatic pancreatic cancer: A prospective, multicenter, single-arm, phase 2 study. Journal of Clinical Oncology. 2024;42(Suppl 16):4135.
-
RCT-PAAG Study. ClinicalTrials.gov Identifier: NCT06051851
-
PAAG randomized data presented at 2026 ASCO Gastrointestinal Cancers Symposium, January 8-10, 2026.
-
National Comprehensive Cancer Network. Pancreatic Adenocarcinoma Guidelines, v2.2026.
-
Sohrabi H, Ghavam SM, Azadnajafabad S, Rezaei N. Efficacy and Safety of Combination Therapy With Immune Checkpoint Inhibitors and Chemotherapy with Gemcitabine and Nab-Paclitaxel in Pancreatic Cancer: A Systematic Review. Cancer Medicine. 2026;15(2):e71637.
-
Park W, Chawla A, O’Reilly EM. Pancreatic Cancer: A Review. JAMA. 2021;326(9):851-862. doi:10.1001/jama.2021.13027.
This article is for educational purposes and does not constitute medical advice. Patients should consult their healthcare providers for personalized treatment recommendations. Data presented reflects results as of the publication dates cited above.